



$740.00
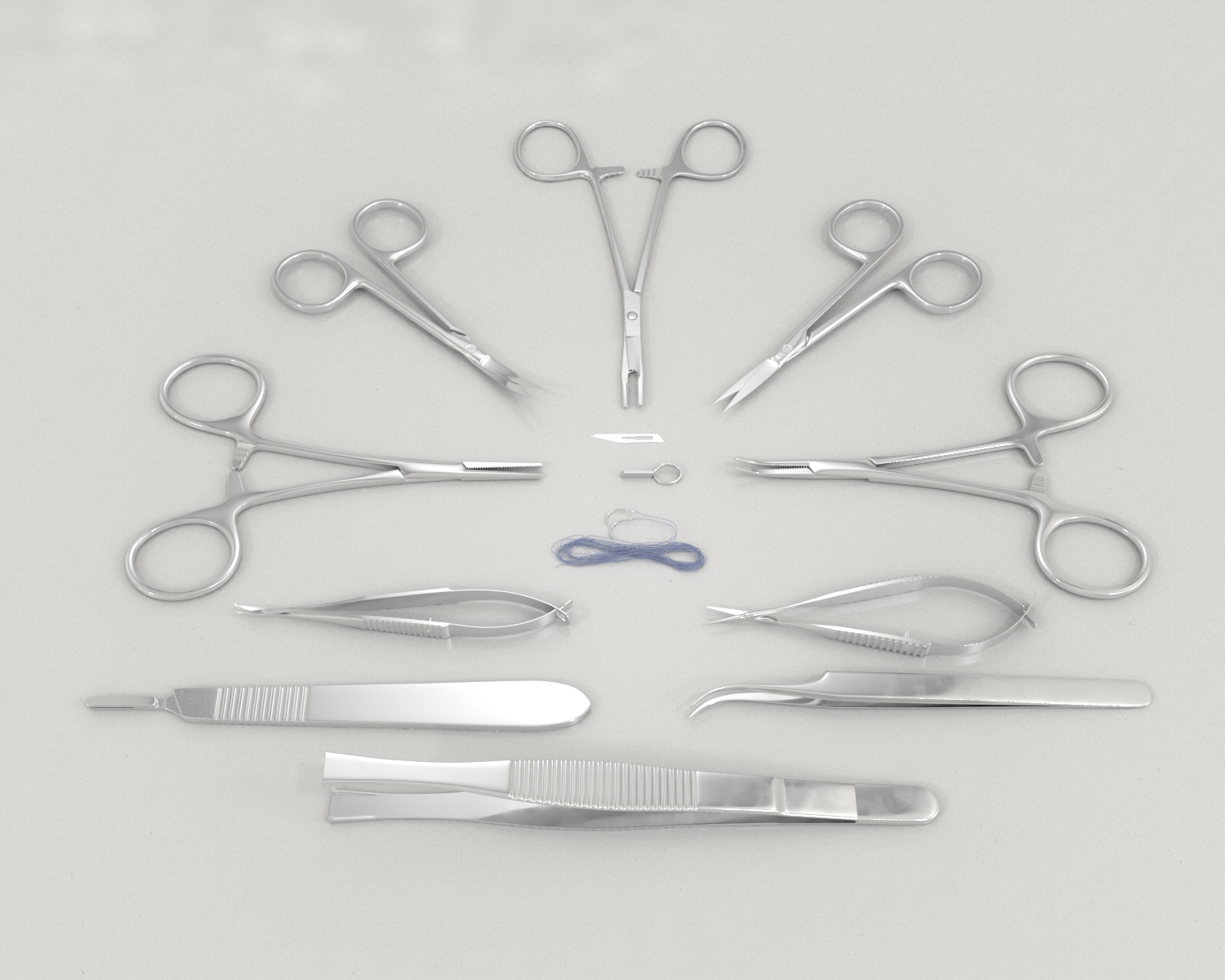
Microsurgery is performed under magnification employing advanced diploscopes, specialized precision tools, and various operating procedures, based on delicate manipulation of microstructures that require highly precise and reliable instruments.
The microsurgical methods are primarily used for vascular anastomosis, nerve coaptation, tissue transplantation, and reattachment of the amputated body parts of the rodents.
Conduct Science offer Microsurgery Kits.

RWD is a global leader in the design and manufacturing of advanced research and laboratory equipment. Specializing in high-precision instruments for neuroscience, behavioral science, and pharmacology.























| SKU | Description | Quantity |
|---|---|---|
| RWD-S12005-10 | IRIS-Fine fine cut-straight / pointed & pointed/10.5cm | 1 |
| RWD-S12004-09 | IRIS-Fine Fine Cut-Bend/Pointed&Pointed/9.5cm | 1 |
| RWD-F31047-12 | OLSEN-HEGAR Needle Holder (Cut)-Straight/2.15mm Width/12cm | 1 |
| RWD-F11001-11 | Fine tweezers-straight/tip 0.2*0.12mm/11cm | 1 |
| RWD-R31005-04 | Stainless steel micro-vascular clamp-straight/4*0.75mm/16mm | 5 |
| RWD-R34001-14 | Vascular clamp holder-with stainless steel micro-vascular clamp/14cm | 1 |
| RWD-S11001-08 | VANNAS Spring Shear-Straight/Mitsubishi/Pointed&Pointed/8cm | 1 |
| RWD-S11002-08 | VANNAS spring shear-bent/mitsubishi/pointed&pointed/8cm | 1 |
| RWD-F22002-10 | HARTMAN mosquito hemostatic forceps-straight / 0.8mm wide / 10.5cm | 1 |
| RWD-F22003-10 | HARTMAN Mosquito Hemostat-Curved/1mm Width/10cm | 1 |
| RWD-F35401-50 | Non-absorbent polyester suture (with needle) -3/8 round needle / 5-0 (50/box) | 0.2 |
| RWD-S32003-12 | Scalpel handle 3# (with ruler) -12.5cm | 1 |
| RWD-S31011-01 | Surgical blade-11# (box x 100 pieces/box) | 1 |
| RWD-SP0000-P | Surgical instrument bag-32*22cm | 1 |
| SKU | Description | Quantity |
|---|---|---|
| RWD-S12005-10 | IRIS-Fine fine cut-straight / pointed & pointed/10.5cm | 1 |
| RWD-S12004-09 | IRIS-Fine Fine Cut-Bend/Pointed&Pointed/9.5cm | 1 |
| RWD-F31047-12 | OLSEN-HEGAR Needle Holder (Cut)-Straight/2.15mm Width/12cm | 1 |
| RWD-F11001-11 | Fine tweezers-straight/tip 0.2*0.12mm/11cm | 1 |
| RWD-R31005-04 | Stainless steel micro-vascular clamp-straight/4*0.75mm/16mm | 5 |
| RWD-R34001-14 | Vascular clamp holder-with stainless steel micro-vascular clamp/14cm | 1 |
| RWD-S11001-08 | VANNAS Spring Shear-Straight/Mitsubishi/Pointed&Pointed/8cm | 1 |
| RWD-S11002-08 | VANNAS spring shear-bent/mitsubishi/pointed&pointed/8cm | 1 |
| RWD-F22002-10 | HARTMAN mosquito hemostatic forceps-straight / 0.8mm wide / 10.5cm | 1 |
| RWD-F22003-10 | HARTMAN Mosquito Hemostat-Curved/1mm Width/10cm | 1 |
| RWD-F35401-50 | Non-absorbent polyester suture (with needle) -3/8 round needle / 5-0 (50/box) | 0.2 |
| RWD-S32003-12 | Scalpel handle 3# (with ruler) -12.5cm | 1 |
| RWD-S31011-01 | Surgical blade-11# (box x 100 pieces/box) | 1 |
| RWD-SP0000-P | Surgical instrument bag-32*22cm | 1 |
Microsurgery is performed under magnification employing advanced diploscopes, specialized precision tools, and various operating procedures. The microsurgical methods are primarily used for tissue transplantation and reattachment of the amputated body parts of the rodents.
The introduction of the operating microscope made microsurgical procedures more comfortable, and with it, microsurgery involving tissue transplantation began. In the 1960s, the microsurgical techniques gained popularity as the rabbit’s ear was replanted using a microsurgical procedure, which was a remarkable achievement in the discipline of microsurgery since the vessels anastomosed were small. The success of the procedure during the 1960s further strengthened the microsurgical composite tissue transfer techniques in the 1970s. During the next decade, autologous tissue transplantation was introduced. The success of the procedures over the years made microsurgery a significant procedure in rodent surgery. Shorter breeding cycles, faster regeneration, lower costs, and easier handling make rodents ideal for microsurgery research.
Physically examine the animals before starting the surgical procedure. Animals should be monitored for nutritional status, quality of fur (thinning, dirty), and behavior (movements of the limbs and trunk, abnormal gait, rigid walking, and a flat abdomen as a sign of pain). Also, inspect the natural orifices for discharge from the nose, increased salivation, and impurities around the anus and genitals, and observe the condition of the eyes. It is also essential to monitor the breathing pattern because non-manifesting subclinical pulmonary diseases can lead to severe respiratory failure in general anesthesia with subsequent death of the animal.
Pre-anesthetic medications can be applied to prevent bradycardia and suppress bronchoconstriction. Rat’s liver produces atropine esterase, which may resist the atropine effect; therefore repeated injections might be required. Anesthesia is usually induced in the subject with the help of anesthetic systems using a face mask or an anesthetic chamber. Select the appropriate dose and duration of the anesthetic agent depending on the weight of the animal. Once the anesthesia is induced, assess the depth of anesthesia using the toe pinch test. Monitor the subjects for physiological parameters throughout the surgical procedures to ensure that the anesthesia is effective.
Follow the recipient preparation steps mentioned above with the only difference in the inferior vena cava preparation. Do not anastomose the inferior vena cava and do not clean or ligate the branches of the inferior vena cava.
Orotracheally intubate and mechanically ventilate all the animals, using the same respirator and ventilation management as for donor animals. With the recipient animal positioned for a left thoracotomy, shave the left lateral thorax and clean it with a 75% alcohol solution.
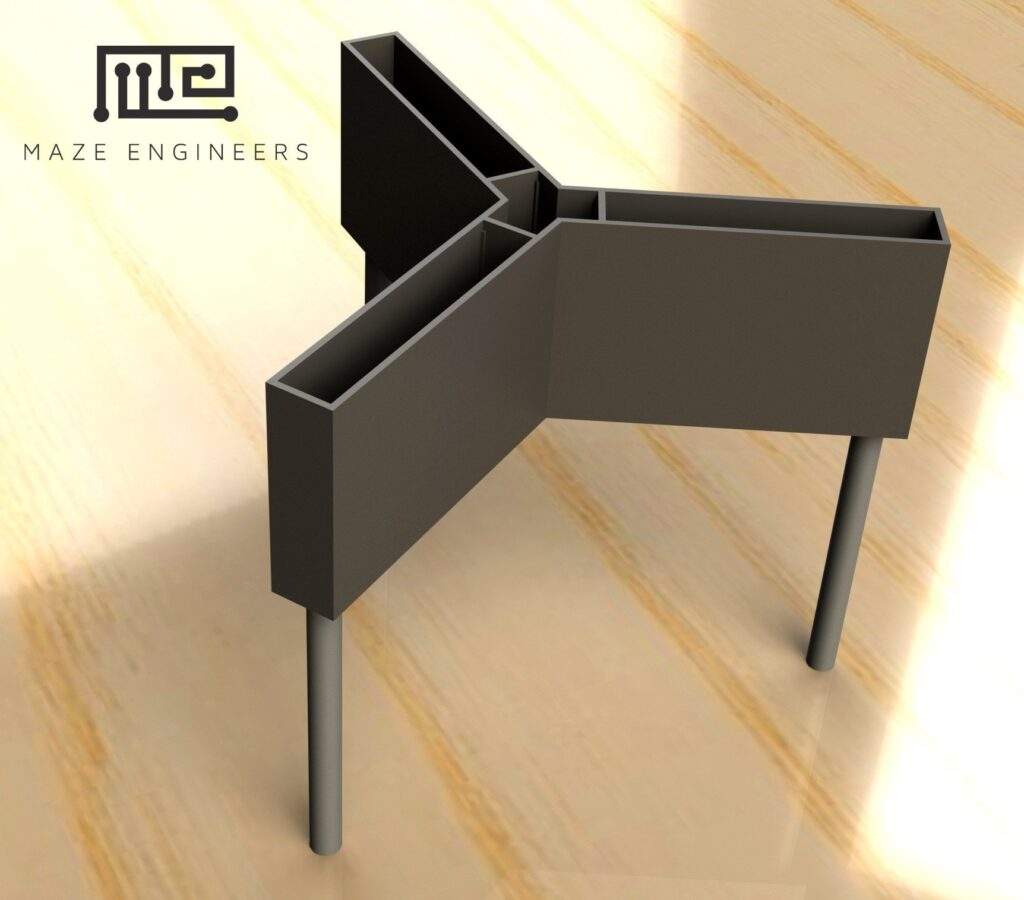
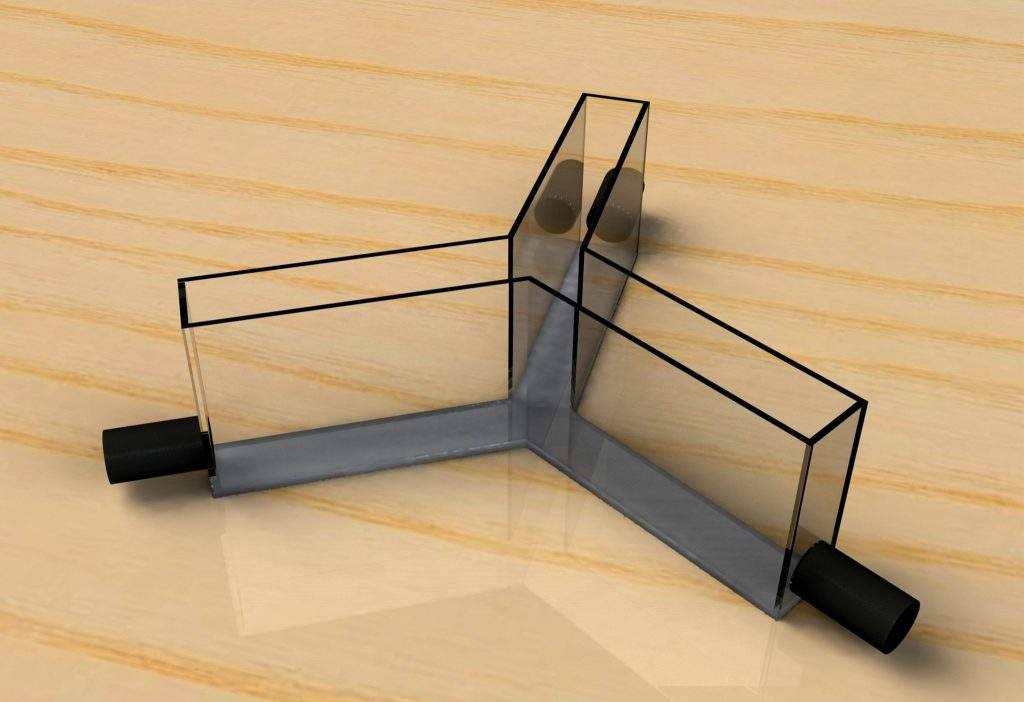
An aluminum plate probed with an L-shaped 2 mm steel wire serves as a base for a 15 cm long steel cylinder. To allow vertical movement in the cylinder, tap the cylinder on the side. Mount a mosquito clamp on top and anchor it with an articulated joint. Intraoperatively, attach an aneurysm clip clamping the cuffed vessels and the recipient bronchus during anastomosis to the mosquito clamp. This construction allows for precise longitudinal movements of the clip on a vertical and horizontal axis as well as rotation on a vertical axis.
Remove the transplanted rat from the ventilator and place the animal under a heat lamp until fully awake.
It is recommended to use heavier and bigger animal recipients. Use rats weighing between 250 and 300g as donors and rats weighing between 300 and 350g as recipient animals, respectively. Almost every recipient animal develops a mild pleural effusion within the first postoperative days. The experimental setting should be favorable for animal survival and be giving a gentle pleural effusion place to expand without compressing other major thoracic organs.
Anesthetize the animals.
Intubate the animals using a 14G intravenous catheter and ventilate mechanically with a small animal ventilator. Transillumination of the neck facilitates quick intubation. Perform all transplantations using a binocular surgery microscope. Place donor animals in a supine position under the operating microscope; place the recipient animals in a right lateral position to allow proper access to the complete left hemithorax.
Oncological surgical techniques and radiotherapy are valuable tools to fight cancer. Regional lymph node dissections, widely used procedures, seem to progress as they result in lesser morbidity and better recovery; they are the most common cause of secondary lymphedema in the industrialized world. Lower limb lymphedema, gynecological malignancies, or upper limb lymphedema, secondary cases to breast cancer treatment, varying from mild to severe benefit from lymphedema surgery. Relatively new, microsurgical techniques are becoming the backbone of surgical lymphedema treatment. The model enables anastomosis of lymphatic structures and numerous available small-caliber veins around the neck. The lymphatic venous anastomoses model created by the microsurgical techniques in the rat provided the researchers with great insight into the surgical treatment of lymphedema.
The microsurgical fallopian tube anastomosis technique is used to restore fertility in women who underwent tubal sterilization or excision of an occluded or diseased portion of the tube. The microsurgical fallopian tube anastomosis procedure restores fertility with excellent results and allows to avoid disadvantages associated with other popular treatment options including in vitro fertilization. The rat uterus possesses unique characteristics making it analogous to the isthmic portion of the human fallopian tube even though the rat’s fallopian tube is highly convoluted and significantly smaller when compared with humans. Female rats possess a duplex uterus consisting of two tube-shaped horns extending upwards toward the kidneys. Each uterine horn has a uniform caliber similar to that of the human oviduct, a thick muscular layer, and mucosa that is not folded abundantly and does not tend to prolapse. The outer serosal layer receives a vascular supply from the broad ligament, which anchors the horn to the dorsal body wall and has a structure highly analogous to the human mesosalpinx. The rat fallopian tube anastomosis provides an excellent model for research and microsurgical procedures.
Reconstructive surgery procedures involving free-tissue transfer are predominantly used in plastic surgery. It was researched that the state of microcirculation and its reaction to changeable conditions plays an important role in these procedures. In the field of ongoing research on microcirculation, various in vitro and in vivo experimental animal models are devised to assess microcirculatory structure, pathophysiology, and hemodynamics. Unquestionably, experimental research employing microcirculation models has considerably contributed to advances in reconstructive and plastic surgery and has improved postoperative prognosis.
Small bowel rat transplantation (SBT) is a cumbersome, time-consuming, and technically demanding procedure with high postoperative mortality in the first seven postoperative days. The small intestine transplantation procedure is either heterotopic or orthotopic with the portal or systematic venous drainage. The crucial factor for animal survival is the time of vascular anastomosis (manipulation time). A threshold of manipulation time of less than 45 minutes is recommended. Microsurgical procedure for small intestine transplantation has significantly reduced the manipulation time thereby increasing the animal survival post-operatively. Microsurgery has provided researchers with a straightforward and more comfortable small intestine transplantation procedure.
The microsurgical groin skin flap model in the rat is accepted widely, as the experimental model offers an inexpensive, practical, and valid instrument and techniques to practice microvascular anastomosis as well as to investigate numerous research questions. The modified rat groin flap employing the inguinal fat pad as an obstacle to minimize the effects of the bed on the skin of the groin flap has further developed the method of the groin skin flap. The standard model of the groin flap and its modifications describe the experimenters about flap design and vascular anatomy. The microsurgical groin skin flap model ensures 100% animal survival for rats post-operatively. The model is not only reliable and reproducible for practicing end-to-end and end-to-side microvascular anastomosis but also a time-saving, less technically demanding, economical, and useful tool to explore numerous research questions that extend from the underlying mechanisms of flap survival to the development of a further surgical design.
As small rodents possess high metabolic activity, do not exceed pre-anesthetic fasting beyond 2 hours. Extended periods of food deprivation can lead to disturbances in balance, metabolic acidosis, and hypoglycemia. During prolonged fasting, essential intestinal flora dies, which may result in the resorption of endotoxin. Water must never be restricted during the pre-anesthetic period. For more comfortable handling the organs in the abdominal cavity, liquid food can be given in place of solid food approximately 8–12 hours before surgery.
Animal handling should be calm and gentle to avoid the intense release of stress which may cause tachyarrhythmia with subsequent cardiac arrest during the general anesthesia. Animal strain and breed must be selected depending on the requirements of the investigation since the subject’s strain affect the experimental results. Also, consider the age and gender of the subject. For pre-operative preparations, the surgical area should be separate from the main surgical site. Thoroughly clean all the equipment and the instruments before starting the surgical procedures. Ensure that the animal is properly anesthetized before beginning the surgery. Avoid damaging the surrounding tissues and muscles during surgical operations.
| Species | Mouse, Rat |
|---|
You must be logged in to post a review.
There are no questions yet. Be the first to ask a question about this product.
Monday – Friday
9 AM – 5 PM EST
DISCLAIMER: ConductScience and affiliate products are NOT designed for human consumption, testing, or clinical utilization. They are designed for pre-clinical utilization only. Customers purchasing apparatus for the purposes of scientific research or veterinary care affirm adherence to applicable regulatory bodies for the country in which their research or care is conducted.
Reviews
There are no reviews yet.